


The VBAC, short for Vaginal Birth After Cesarean Section, describes the vaginal delivery of a baby in a patient who has previously had at least one delivery by Cesarean Section.
Over the past thirty years there has been an enormous amount of controversy regarding this procedure with advocates both "for and against" the VBAC touting its benefits as well as its associated risks.
What has made it all the more confusing to the general public has been the apparent shifts in recommendations "for and against" within the medical community, specifically within the specialty of Obstetrics and Gynecology (OB/GYN).
Since the first month of my residency, back in August 1995, I have been a very strong advocate for the VBAC. My senior residency award research paper titled, "Risk Assessment of Uterine Rupture During Trial of Labor: Evaluation of a VBAC Scoring System," specifically addressed the management of a trial of labor using a scoring system to calculate the probability of a successful vaginal delivery.
After reading thousands of pages of literature on the subject and having performed thousands of normal vaginal deliveries and hundreds of VBACs, I continue to promote the option of the VBAC to my patients.
This website will review the history, risks, benefits and current recommendations regarding the VBAC and hopefully will serve as a guide my patients interested in attempting the VBAC by providing the comprehensive unbiased review and opinion on the subject.
In 1916, Dr. E.B. Cragin delivered an address entitled "Conservatism in Obstetrics" to the Eastern Medical Society of New York in which he coined the phrase "Once a caesarean, always a caesarean."
For most of the twentieth century, doctors followed this dogma believing that once a woman delivered by C/S she should deliver all future pregnancies by repeat C/S. Clinical studies starting the 1960s, however, concluded that this practice was not always necessary.
In 1980, the National Institutes of Health (NIH) Consensus Development Conference Panel questioned the necessity of routine repeat Cesarean Section. After extensive research, the panel made recommendations regarding the VBAC. Their recommendations gave support to the practice of the TOLAC and successful VBAC with a significant rise in the number of attempted VBAC from the 1980s through 1996.
A major turning point occurred in 1996 with a study published in The New England Journal of Medicine (MacMahon et al, 1996) which concluded that a vaginal delivery after previous C/S (VBAC) was associated with an increased maternal complications as compared to the Elective Repeat Cesarean Section (ERCS).
The American College of Obstetrics and Gynecology (ACOG) subsequently issued guidelines in its 1999 Practice Bulletin which recommended that "VBAC should be attempted in institutions equipped to respond to emergencies with physicians immediately available to provide emergency care." (ACOG, 1999) This practice bulletin also recommended that a physician "capable of monitoring labor and performing an emergency cesarean delivery" be "immediately available throughout active labor," and that anesthesia and personnel for an emergency cesarean be "available."
Logistical and professional liability issues led many hospitals to restrict or prohibit the practice of VBAC. As a result, the rate at which VBAC was attempted fell from 26% in the early 1990s to less than 10% today.
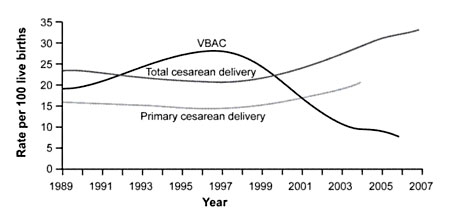
Figure 1. Rates of Total Cesarean Deliveries, Primary Cesarean Deliveries, and Vaginal Birth After Cesarean (VBAC), 1989 to 2007. Data from the National Center for Health Statistics.
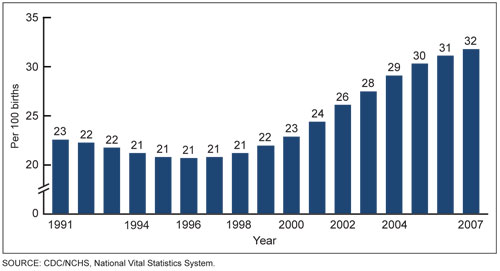
Figure 2. Increasing Rates of Cesarean Section, 1991 to 2007. Data from the US Department of Health and Human Services.
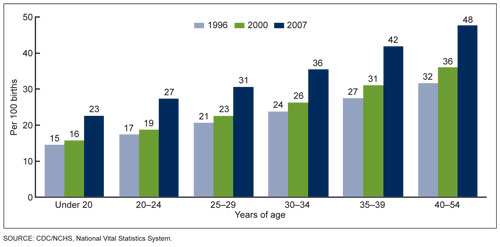
Figure 3. Cesarean delivery rates by age of mother. United States, 1998, 2000 & 2007. Data from the US Department of Health and Human Services.
In March 2010, the National Institutes of Health (NIH) hosted its Consensus Development Conference on the subject of VBAC and concluded, "Given the available evidence, trial of labor is a reasonable option for many pregnant women with one prior low transverse uterine incision.".
Also in March 2010, the U.S. Department of Health and Human Services (HHS), Agency for Healthcare Research and Quality (AHRQ) reported that VBAC is a reasonable and safe choice for the majority of women with a history of prior C/S and that there is emerging evidence of serious harm relating to multiple Cesarean Sections.
In July 2010, The American Congress of Obstetricians and Gynecologists (ACOG) similarly revised their own guidelines to be less restrictive of VBAC, stating, "Attempting a vaginal birth after cesarean (VBAC) is a safe and appropriate choice for most women who have had a prior cesarean delivery, including for some women who have had two previous cesareans."
Dr. Novoa graduated with honors from Meharry Medical School in 1995. He practices a multi-disciplinary "Minimally Invasive Surgery" approach to the management of women's health care.
The Novoa Women & Teen Centers provide expert management of normal and high-risk pregnancy. Dr. Novoa will monitor your health and the health of your baby throughout prenatal and post-partum period.
Our Gynecological services range from well-woman, preventive care to diagnostic and treatment of complex gynecological concerns. For your convenience and comfort, we provide a full range of office gynecological procedures in our warm and friendly office environment. Additionally, Dr. Novoa also offers inpatient and outpatient surgery.
If you have a life-threatening emergency, call 911. If your matter is an emergency (only) and you need to speak to Dr. Novoa concerning this emergency after the office has closed, please call 951.595.9944 (Wait for the prompt and you will be connected to Dr. Novoa). If you have a question that is not an immediate emergency, please call during office hours. A nurse or physician will assist you as soon as possible.

10781 Pebble Hills, Suite A
El Paso, TX 79935
915.595.9944
915.996.9074
Monday - Friday:
9:00am - 5:00pm